


Negative symptoms, neurocognition and work functioning
- For many individuals with severe mental illness, the critical ingredient of recovery is competitive employment.
- Employment/work functioning is impacted hugely by negative symptoms and neurocognition.
- Negative symptoms impact processing speed and through that work functioning in both cross-sectional and prospective data analyses, while neurocognition influenced negative symptoms and indirectly work functioning only in the cross-sectional analyses.
In this section
This longitudinal 20-year prospective study by Luther et al. examined the impact of negative symptoms and neurocognition on work functioning in patients with severe mental illness (SMI). More specifically, authors were interested in clarifying whether (1) neurocognition influences negative symptoms and thereby work functioning or whether (2) negative symptoms influence neurocognition and thereby work functioning.
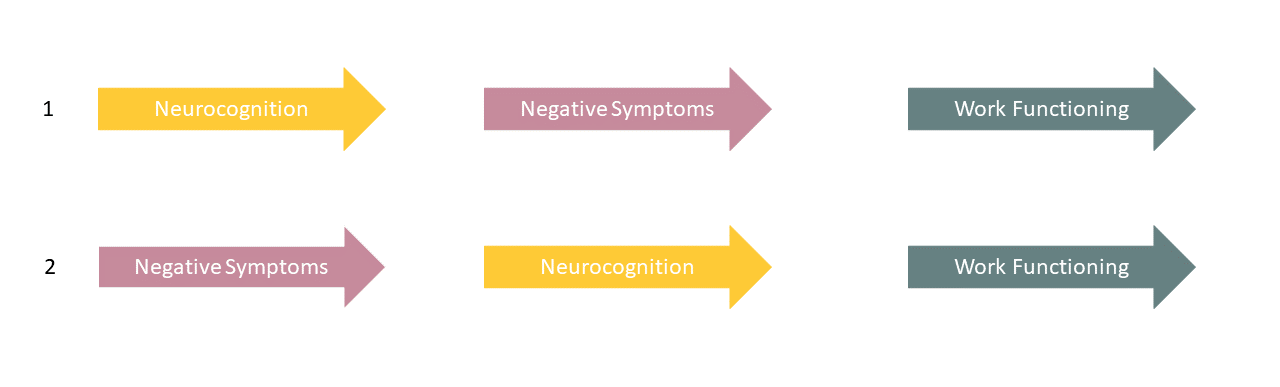
Former literature data has shown that both neurocognition and negative symptoms have strong links to functional outcomes, but that the pathway goes through neurocognition preceding or predicting negative symptoms and as such indirectly influencing functional outcomes via its impact on negative symptoms (pathway 1).The current study sought to also test the opposite hypothesis of whether greater negative symptoms predict reduced neurocognition and indirectly influence work functioning (pathway 2).
To address this issue, the Harrow Chicago Follow-up Study, a longitudinal observational research project, was designed. 277 participants with a SMI with psychotic features were identified and interviewed during an index inpatient hospitalization period, and were assessed 2, 4.5, 7.5, 10, 15 and 20-years later. Assessment scales included negative symptom scales (Behaviour Rating Schedule of the Psychiatric Assessment Interview) and neurocognitive scales (Wechsler Adult Intelligence Scale). Employment status was accessed by the interviewer-rated Strauss and Carpenter outcome scale for working functioning. Both hypotheses were tested using cross-sectional and prospective data analyses.
Results showed that both hypotheses (pathways 1 and 2) were supported by the cross-sectional analyses: neurocognition showed to lead to greater negative symptoms, which in turn lead to reduced functional outcomes; but also greater negative symptoms predicted reduced neurocognition and in turn poor functional outcomes. The former was in line with previous literature data, while the latter was a new finding.
In prospective models, only the second hypothesis (pathway 2) supporting that negative symptoms influenced work functioning through the mediation of neurocognition was true, while the opposite was not true: no evidence was seen that negative symptoms significantly mediated the relationship between neurocognition –either processing speed or general knowledge – and work functioning. Lower neurocognition did not significantly predict greater prospective negative symptoms. In summary, these prospective models offered greater support for a causal pathway running from negative symptoms to neurocognition to work functioning (pathway 2).
Authors further emphasized that negative symptoms such as apathy likely influence neurocognition, specifically processing speed. The longer the negative symptoms exist, the more they contribute to reduced neurocognitive resources. This reduction may in turn lead to poorer performance at work. Processing speed was observed to be a stronger predictor of work functioning than general knowledge in both cross-sectional and prospective models. Finally, positive symptoms also predicted work functioning in all cross-sectional and prospective analyses.
For many individuals with SMI, the critical ingredient of recovery is competitive employment, but unfortunately, treatments have not yet been able to efficiently improve work functioning, the article points out. Findings suggest that targeting negative symptoms prior to neurocognition could be more beneficial for long-term work outcomes, as improving negative symptoms could improve processing speed and general knowledge and in turn work functioning. Targeting negative symptoms with interventions such as CBT, Metacognitive Reflection and Insight Therapy, or repetitive transcranial magnetic stimulation may directly as well as indirectly improve subsequent work functioning. Also, combining treatments with cognitive remediation that specifically targets processing speed might be beneficial.
Schizophrenia Research
Clarifying the direction of impact of negative symptoms and neurocognition on prospective work functioning in psychosis: A 20-year longitudinal study
https://doi.org/10.1016/j.schres.2020.03.012
CHALLENGES OF THE COVID-19 PANDEMIC CHALLENGES OF THE COVID-19 PANDEMIC
Nowadays, the target for the treatment of people with schizophrenia is not simply the remission of positive symptoms, but also functional remission bringing Nowadays, the target for the treatment of people with schizophrenia is not simply the remission of positive symptoms, but also functional remission bringing
more...DRUG-NAÏVE FEMALE PATIENT DRUG-NAÏVE FEMALE PATIENT
(COD. 300020/R34. Submitted to AIFA on 12 October 2020). This is a case report describing a 52-week Reagila treatment regimen that follows the impressive This is a case report describing a 52-week our product treatment regimen that follows the impressive clinical improvement of a patient with an early onset of
more...